
Disclaimer: I’m not an attorney, this is not legal advice.
Overview
With the exponential increase in the United States for regenerative procedures over the past decade, there has also been a major rise in regulatory questions. These questions revolve around autologous vs allogeneic regulations, cellular vs acellular and whether or not full FDA approval is required for marketing and/or usage of products.
In July of 2020, the FDA published a Regulatory handbook in an attempt to address a lot of the questions. Unfortunately, many industry competitors such as sales reps and company owners have either not read the handbook, or just decided to disseminate false information about the regulations.
Here’s the header of the handbook:
FDA Responsibility
Hopefully this article will clear up how these tissues are actually regulated. The USA FDA has jurisdiction in America over human and veterinary drugs, biological/tissue products and medical devices. The goal is to ensure the highest level of safety, effectiveness and security possible for these as well as the nation’s food supply and cosmetics too.
While the FDA regulates drugs, biologics, tissues and devices from a manufacturing and marketing perspective, they do NOT regulate the practice of medicine in the USA. A lot of people do not realize that. That responsibility lies with each state’s medical board.
When a medical provider is sitting in a consultation with a patient, and a decision is made to use a technology for treatment, the FDA has nothing to do with that conversation.
Autologous vs Allogeneic
If a medical provider performs a procedure using a patient’s own bone marrow or adipose tissue, and then delivers that tissue back to the patient, that is an autologous procedure. If a medical provider uses tissue from a donor to place into a patient, that is an allogeneic procedure.
Interestingly, the FDA in America tries to look at these tissues with the same set of regulations. While some providers have looked at autologous procedures as being a “free for all” with how they are used, that is not the case! Having one set of regulations has leveled the playing field between usage.
FDA’s Categorizations 351 vs 361
These FDA regulations place tissue into one of two categories under the Public Health Service Act, which is part of the Code of Federal Regulations Part 1271. The division of the FDA tasked with the regulatory authority is known as CBER, which stands for Center for Biologics Evaluation and Research. They have separated tissues and biologics into two categories, either as a 351 or a 361 designation.
If a tissue is designated as a 351 product, then it falls into the drug/biologics pathway. This means it requires a series of Clinical Trials to obtain full FDA Approval for usage. Just like a drug, once the biologic is approved it will then be approved for marketing for a specific therapeutic use. Any other use would be considered “off label”. “Off label” usage is very common in the USA.
Now let’s discuss the 361 designation. In the July 2020 FDA Regulatory handbook, they mention that in order to qualify as a 361 tissue product, the criteria of both “minimal manipulation” and “homologous use” need to be met.
I’ll define those specifically in a moment. If both of those criteria are met, the tissue achieves the designation of an HCT/P. That is short for Human Cells, Tissues, and Cellular and Tissue-Based Products.
See the table below, which distinguishes the two categories.
Minimal Manipulation
Alright so let’s define Minimal Manipulation. This has to do with the methods by which the tissue is processed, whether it’s autograft or allograft. Per the FDA’s Regulatory handbook, minimal manipulation refers to the following:
- For structural tissue, processing that does not alter the original relevant characteristics of the tissue relating to the tissue’s utility for reconstruction, repair, or replacement
- For cells or nonstructural tissues, processing that does not alter the relevant biological characteristics of cells or tissues.
In the handbook, the FDA lists examples of structural tissues including:
- Bone
- Skin
- Amniotic membrane and umbilical cord
- Blood Vessel,
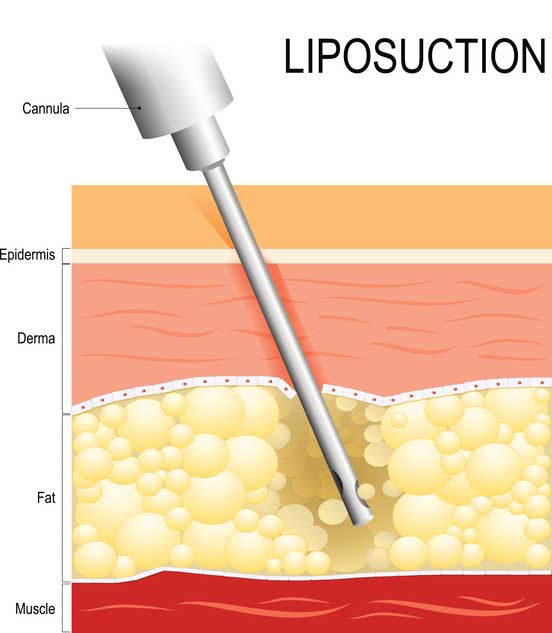
- Adipose Tissue
- Articular cartilage
- Non-articular cartilage
- Tendon or ligament
The FDA provides several examples of ways a processing lab or medical provider could deviate from Minimal Manipulation. One allograft example is “a manufacturer grinds and lyophilizes amniotic membrane and packages it as particles. The HCT/P generally is considered more than minimally manipulated because the processing alters the original relevant characteristics of the HCT/P relating to its utility to serve as a barrier”.
Another example, which involves autograft, involves the Adipose Stromal Vascular Fraction (SVF) procedure. The processing for SVF involves adding the enzyme collagenase to break down the tissue. The FDA considers this more than minimal manipulation, as “the processing breaks down and eliminates the adipocytes and the surrounding structural components that provide cushioning and support, thereby altering the original relevant characteristics”.
Umbilical cord tissue has been designated by the FDA as a structural tissue. By a lab processing umbilical tissue carefully and not using enzymes, culturing or anything that alters the tissue’s utility for reconstruction, repair, or replacement, then it remains a minimal manipulation tissue.
Homologous Use
When it comes to homologous use, there is a difference between the scientific definition and the regulatory one. Scientifically it’s very simple – homologous means using tissue from one species into the same. So tissue from a human would be going into another one. But that’s not what the FDA is referring to!
What the FDA refers to with homologous use is this. “Homologous use means the repair, reconstruction, replacement, or supplementation of a recipient’s cells or tissues with an HCT/P that performs the same basic function or functions in the recipient as in the donor, including when such cells or tissues are for autologous use.”
So keep in mind right off the bat is that the FDA includes autologous and allogeneic procedures together in this, meaning it could be “recipient” or “recipient site”. The function needs to be consistent from the donor to the recipient. They go on to state the following.
- Recipient cells or tissues that are identical (e.g., skin for skin) to the donor cells or tissues, and perform one or more of the same basic functions in the recipient as the cells or tissues performed in the donor; or,
- Recipient cells or tissues that may not be identical to the donor’s cells or tissues, but that perform one or more of the same basic functions in the recipient as the cells or tissues performed in the donor.
One example provided is that of, “an amniotic membrane product is applied to the surface of the eye to cover or offer protection from the surrounding environment in ocular repair and reconstruction procedures. This is homologous use because serving as a covering and offering protection from the surrounding environment are basic functions of amniotic membrane.”
If a medical provider uses either autograft adipose (not SVF) or allograft umbilical cord in a patient for structural support of a joint, homologous use applies. The tissue is providing cushioning, protection and lubrication, which is the same as it does in the donor, or donor site in the autograft procedure.
Misinterpretations and Clarifications
There are two points of clarification that need to be made with the homologous use classification. One involves the presence of live cells in a tissue product.
A lot of competitors have stated that the presence of live cells automatically changes a tissue product from a 361 to a 351. This is not true! It’s not a grey zone, as the FDA wrote about it directly in the 361 description. Here it is:
Section 4 i) states that the tissue should not have a systemic effect or be dependent on the metabolic activity of living cells for its primary function. It does not say “any function”. So in addition to providing structural support, the HCTP can, in fact, have live cells in it that serve a secondary local metabolic function.
In 4 ii) the FDA also states that autologous use procedures may actually have a systemic effect, or be dependent upon the metabolic activity of living cells for its primary function. So that is a significant difference between autologous and allogeneic procedures.
The second point of clarification is whether or not any live cells in an HCTP can serve a function. The answer is yes! As shown above, for allogeneic procedures, it needs to be a secondary, local metabolic function.
Conclusion

In order to be categorized as a 361 HCT/P, a tissue product needs to meet the FDA’s definition of both minimal manipulation and homologous
use. Both autologous and allogeneic tissue need to meet these criteria, but they are a bit less strenuous for autologous with regards to being able to serve a systemic function.
It’s been disheartening and disingenuous for competitors to twist the FDA’s regulations to suit their narrative. Umbilical cord tissue products can definitely meet the criteria as a 361 HCT/P, as long no “therapeutic claims” are being made by the manufacturer or overtly in the marketing process. They also are allowed to contain live cells, as long as those cells are only serving a secondary function with a local metabolic nature.
Keep in mind that NONE of the FDA’s publication concerns what a discussion entails between a medical provider and his/her patient. That involves the practice of medicine, and the FDA does not regulate that.
If you would like to find out more information about the top umbilical cord Wharton’s Jelly HCTP available that is FDA 361 Compliant, contact Regen Suppliers today about ReBellaWJ at (888) 568-6909. Or simply visit https://rebellabiologic.com/product/rebellawj/ for more information.
Here’s a couple videos I’ve done on the topic as well:
Sorry, the comment form is closed at this time.