The EDSS scale ranges from 0 to 10 in 0.5 unit increments that represent higher levels of disability. Scoring is based on an examination by a neurologist.
In a 2009 Panama study of 20 patients with MS (relapsing-remitting, primary or secondary progressive), patients received intravenous infusions of umbilical cord mesenchymal stem cells.
Enrolled subjects received 140 million umbilical cord mesenchymal stem cells (UCMSC) intravenously over the course of seven visits (20 million stem cells each) separated by 1–4 days. In our case, the statistically significant (p < 0.03) change in EDSS mean scores from baseline to 1 month reflects a change in disability category, which could translate into an improved ability to walk and work a full day with minimal, if any, assistance. The intravenous infusion of UCMSC over several days is safe in subjects with MS.
Additionally, UCMSC infusions may hold benefits, since this small study group saw improvement in bladder, bowel, and sexual dysfunction, walking, upper extremity physical function, energy and fatigue, general perspective of a positive health change and improved quality of life, and MRI lesions. Most subjects (83.3%) showed no disease progression or new lesions in their MRIs.
In 2022, a case report was published of an MS patient treated for 11 years, with multiple infusions of MSCs derived from either his bone marrow (BM), pooled human umbilical cords (UC), or from his own child umbilical cord. The mesenchymal stem cell (MSC) treatment was well tolerated with no significant side effects.
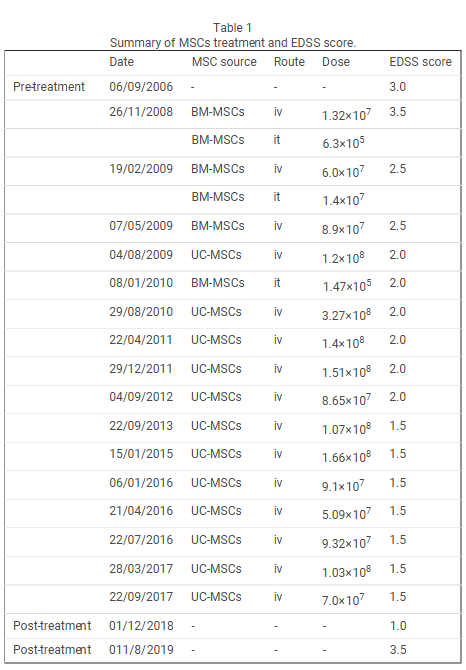
A 27-year-old male started treatment in 2008, who was diagnosed as relapsing remitting MS From 2008 to January 2010, he received 3 intravenously as well as 3 intrathecal infusion of BM-MSCs. As the patient stabilized, UC-MSCs were subsequently used for the transplantation. From August 2009 to December 2018, he received a total of 12 intravenous infusions of UC-MSCs, in the absence of any other disease-modifying therapy (DMT).
They looked at the long term effect of multiple MSCs infusions in an MS patients to a period of some 11 years. It is noteworthy that following the MSC treatment, the patient with a progressive MS, showed a significant improvement in his EDSS score over time and this was in the absence of any disease-modifying therapy (eg, glucocorticoid pulse). The treatment which consisted of 16 MSCs infusions, administrated over more than a decade period, was overall well tolerated and led to an apparent clinical and radiological disease recovery. Indeed, the MRI examinations performed from 2008 until 2018, confirmed the absence of subclinical disease activity, a finding in agreement with other MSCs transplantation studies in MS.
Of particular note is the continuous improvement we witnessed over the 10 years of treatment both clinically and pathologically. The table below details his EDSS score improvements.
A 2018 study published out of China evaluated two patients with multiple sclerosis, who received several mesenchymal stem cell infusions over a two year period.
Intravenous transfusions were performed with 1 to 2 million stem cells/kg at 3-month intervals for 7 times.
Patients in the treatment group received seven times of UCMSCs treatments. During that period of time, they didn’t undergo other drug treatments. The patients in the control group (2 additional patients) continued those medications they had already been taking, including methylprednisolone, glucocorticoid hormones, interferon, human immunoglobulin, neurotrophic factor, and traditional Chinese medicines. However, their conditions were still progressively aggravated.